Crash Course: CPAP vs BIPAP – How It Works
We will cover CPAP and BiPAP, two non-invasive ventilation methods that have become increasingly important in clinical practice, especially given the current situation. This post is designed to provide a comprehensive overview of these methods and help understand how they treat respiratory failure. Given the current situation and recent events, I have received many questions
We will cover CPAP and BiPAP, two non-invasive ventilation methods that have become increasingly important in clinical practice, especially given the current situation. This post is designed to provide a comprehensive overview of these methods and help understand how they treat respiratory failure.
Given the current situation and recent events, I have received many questions from juniors about CPAP and BiPAP. This post is an overview to help understand these non-invasive ventilation methods in clinical practice and is not intended for exam revision.
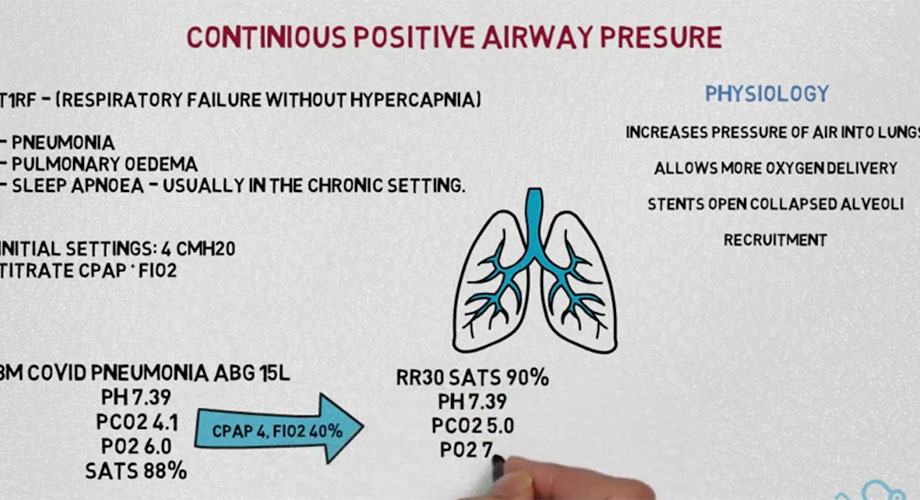

CPAP stands for Continuous Positive Airway Pressure. It is a machine that delivers constant pressure to the lungs during both inhalation and exhalation, providing more oxygen than can be delivered through a regular face mask. The indications for use are clear, with CPAP typically used for worsening type 1 respiratory condition.
Respiratory failure with high CO2 is often treated with CPAP if other medications or medical interventions have failed. Common indications for use include pneumonia, pulmonary edema, and sleep apnea (often in a chronic setting).
CPAP increases the pressure delivered to the lungs, thereby increasing oxygen production. Physiologically, this helps to keep the alveoli open, particularly in cases where they have become closed due to inflammation and scarring from conditions such as pneumonia or pulmonary edema.
CPAP delivers positive pressure to the lungs, which helps keep the alveoli open during exhalation and increases oxygen exchange. This process is called recruitment.
For those not trained as respiratory physicians or who are not experts in the field, it is essential to know that CPAP settings should typically be started at 4. And titrated up or down as necessary to maintain target stats and pO2 levels. Patients will need ongoing respiratory and cardiac monitoring. They may require repeated ABG or SATs to monitor their oxygenation levels.
Some machines use PEEP (Positive End-Expiratory Pressure) instead of CPAP. Just remember to keep monitoring the patient and make adjustments as needed.
For example, consider an 88-year-old man with proven COPD pneumonia. Despite receiving optimal medical treatment, his arterial blood gas results showed a pH of 7.39, CO2 of 4.1, PO2 of 6.0, and saturation of 88%. To improve his condition, you started him on CPAP with a setting of 4 and a FiO2 of 40%. After monitoring his stats, you observed improvement with a saturation of 90%, but his respiratory rate was still 30 breaths per minute. You increased his CPAP to 6 and FiO2 to 40% to further stabilize his condition. His respiratory rate decreased to 25 breaths per minute with a saturation of 96%.
Now, let’s move on to BIPAP (also called NIV), used for respiratory failure with hypercapnia (type 2 respiratory failure). This treatment is commonly used in patients with COPD or a neurological disorder that causes ventilation difficulties, such as those with motor neuron disease.
Indications for using BiPAP include severe respiratory failure with high CO2 levels and low pH, despite optimal medical management or for patients who have been weaned off from mechanical ventilation. The critical difference between BiPAP and CPAP is that it uses two different pressures. An inspiratory positive airway pressure (IPAP). An expiratory positive airway pressure (EPAP). This is useful in conditions like COPD, where elasticity is lost, and CO2 levels are high, causing acidity in the blood’s pH.
To overcome this, IPAP helps by increasing the lung’s forced residual capacity, increasing the rate of diffusion from the blood to the lung, and reducing resistance in the respiratory muscles. This ultimately helps remove CO2 from the blood and allows the patient to ventilate more effectively. EPAP helps increase oxygen delivery by keeping alveoli open and re-expanding the lungs during expiration.
According to the British Thoracic Society, it is recommended to start IPAP at 10 and increase it in 2-interval increments. EPAP is usually set at 4. Monitoring response involves taking arterial blood gas after one hour, four hours, and 24 hours after changing settings. Weaning off BiPAP is often slower and takes breaks for a few hours.
A practical example: We have a patient with COPD who has had an exacerbation causing type 2 respiratory failure that is not responding to first-line measures. BIPAP is indicated due to blood gas showing a pH of 7.23, CO2 of 10.0, and PO2 of 6.6. The patient is started on IPAP of 10 and EPAP of 4. After an hour, the blood gas shows a pH of 7.25, CO2 of 8.9, and PO2 of 6.6, indicating improvement but not enough. The settings are adjusted to IPAP 14 and EPAP 5. After another hour, the blood gas shows a pH of 7.37, PCO2 of 6.6, and PO2 of 8.9. The patient is now improving. Monitor the patient’s cardiac and respiratory status and repeat the blood gas. If the patient deteriorates, consider intubation and ventilation. BIPAP and CPAP should not be used if there’s a risk of aspiration, low GCS, undrained pneumothorax, recent GI surgery, or blatant GI obstruction. Follow local policy and guidance from seniors. This post is not for revision purposes but for practical use in real-life patient care.
Conclusion
In conclusion, CPAP and BiPAP are important non-invasive ventilation methods that have become increasingly used in clinical practice for treating respiratory failure. Understanding their indications, settings, and practical applications is crucial for physicians and healthcare professionals who are not experts in the field. These methods are effective in increasing oxygen delivery. Still, they should not be used if there is a risk of further compromising the patient’s condition. Monitoring and adjustments must ensure the patient’s respiratory and cardiac status remains stable.
Related Posts
What's The Difference of CPAP Mask Types?
What's The Difference of CPAP Mask Types? Here is our Types of CPAP Mask article! We'll examine the main options: full face, nasal, and nasal pillow to help you find the best CPAP mask type for you.
The Best Way to Clean Your Home CPAP Machine
When a home CPAP machine is used for a long time, it needs to be cleaned regularly to keep it clean and free from contamination. Properly cleaning a ventilator can effectively prevent the growth and spread of bacteria while ensuring you breathe cleaner air. Next, BreatheHelp looks at the best way to clean your CPAP
CPAP Machine Problems You Have to Know
We all understand that non-invasive CPAP machines can safely and effectively relieve sleep apnea. Still, we always feel a little uncomfortable wearing a CPAP machine to sleep at night. We collect some of the most common problems encountered by CPAP machine customers. This article tells you how to solve these problems so you can get
Notice: Internet users spontaneously contributed the article content, and the article views only represent the author himself. This site only provides storage services, does not have ownership, and bears relevant legal liabilities. If you find plagiarism, infringement, or illegal content, please contact the administrator to delete it.